delta dental appeal form
Use this form to update the status of your practice as a DeltaCare provider. The Appeal Request Form must be received by Delta Dental of Kansas within 180 calendar days from the date of the original adverse benefit determination or the corresponding remittance.
![]()
Understanding Your Explanation Of Benefits Eob Delta Dental Of Illinois
Electronically submit claims send attachments and retrieve eligibility and benefits with Claim ServicesStreamline.

. INSTEAD you may submit a request for a Stage 1 UM Appeal Review to appeal such determinations. We cover more Americans than any other dental benefits provider - and strive to make dental coverage more. To view benefit information.
Delta Dental requires providers use a resubmission request by selecting that option on this form to resubmit claims for clerical corrections or to provide additional information to support the. You can file a grievance by doing one of the following. This form is not needed for.
Use this secure form to file a grievance or appeal a dental benefits decision. Please refer to the vision appeals packet for information on submitting DeltaVision Administered by EyeMed. How Do I File a Grievance.
Dental rather than medical. Customer Service hours will be from 800 AM 1100 AM ET while our team volunteers and makes an impact in our community. For more information contact 877-585-5731.
Delta Dental of Arkansas. Find solutions that make it easier to manage your practice like benefit information and claims status. Please register with DentalXChange to add new services.
Delta Dental PPO participation packet request. THE PO BOX IS FOR CLAIMS ONLY. Call toll-free at 1-866-864.
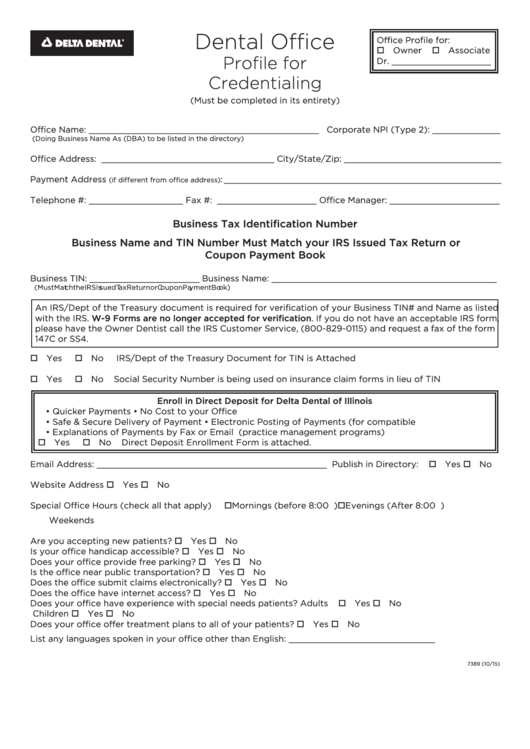
Dentist Administrative Forms and Resources. Delta Dental is Americas largest and most trusted dental benefits carrier. DeltaCare Specialty Referral Form Use this form to refer your patient to a specialist.
CLAIMS APPEALS SHOULD BE SENT TO THE STREET ADDRESS BELOW NOT THE PO BOX. How to Know When You Can Appeal When Delta Dental. Questions about the appeals process you may call the Departments Consumer Assistance Office at 602 3642499 or 8003252548.
On Friday October 7 2022. Locum tenens provider form.

Provider Forms Resources Delta Dental Of Arkansas
Ppo Plus Premier
Delta Dental Provider Dispute Form Pdf Form Udlvirtual Edu Pe
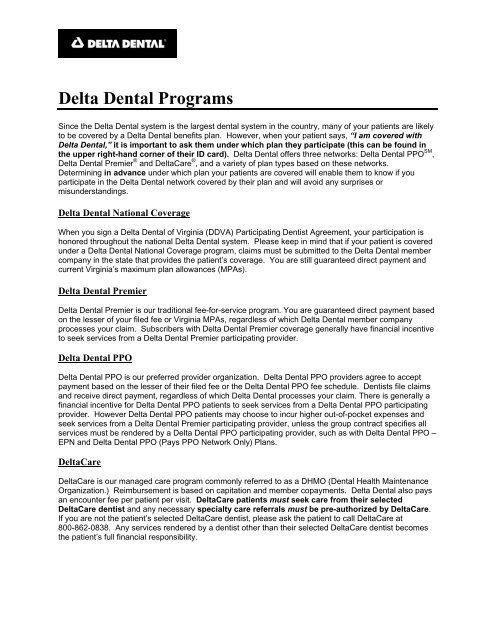
Delta Dental Programs Delta Dental Of Virginia
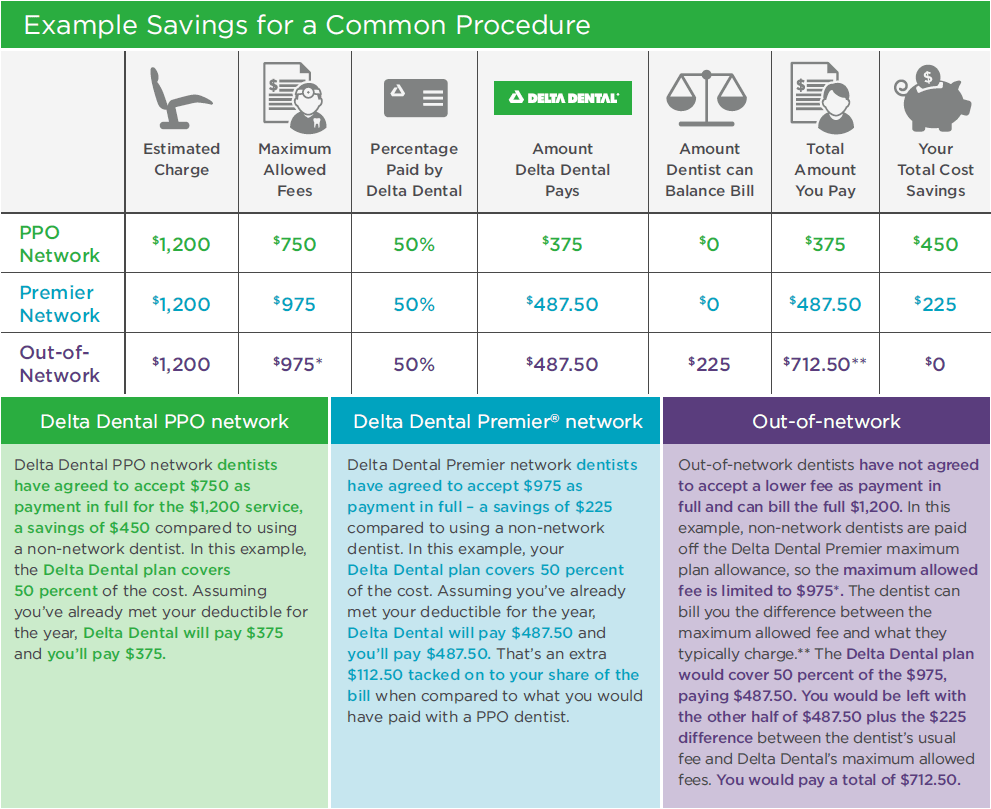
Save Money With Delta Dental Ppo Dentists Delta Dental Of Illinois

Faqs Provider Delta Dental Of Washington Delta Dental Of Washington

Sample Letters Of Appeal To Dental Insurance Lovetoknow
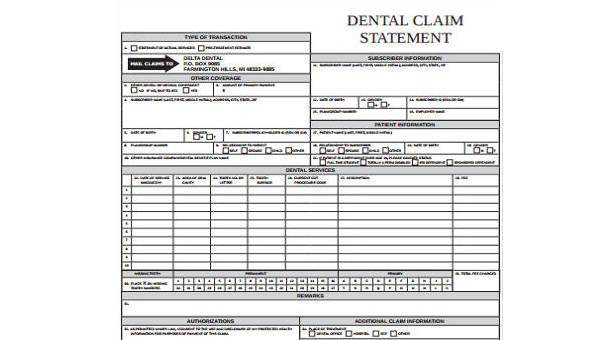
Free 8 Dental Claim Forms Samples In Ms Word Pdf

Member Forms And Downloads Minnesota

Delta Dental 101

Member Forms And Downloads Minnesota

Site Partner Information
Delta Dental Of Arkansas Form Fill Out And Sign Printable Pdf Template Signnow
Delta Dental Michigan Appointment Of Representative Forms

Appeals Grievances Delta Dental Of Arizona

Delta Dental Of Oregon Forms For Members
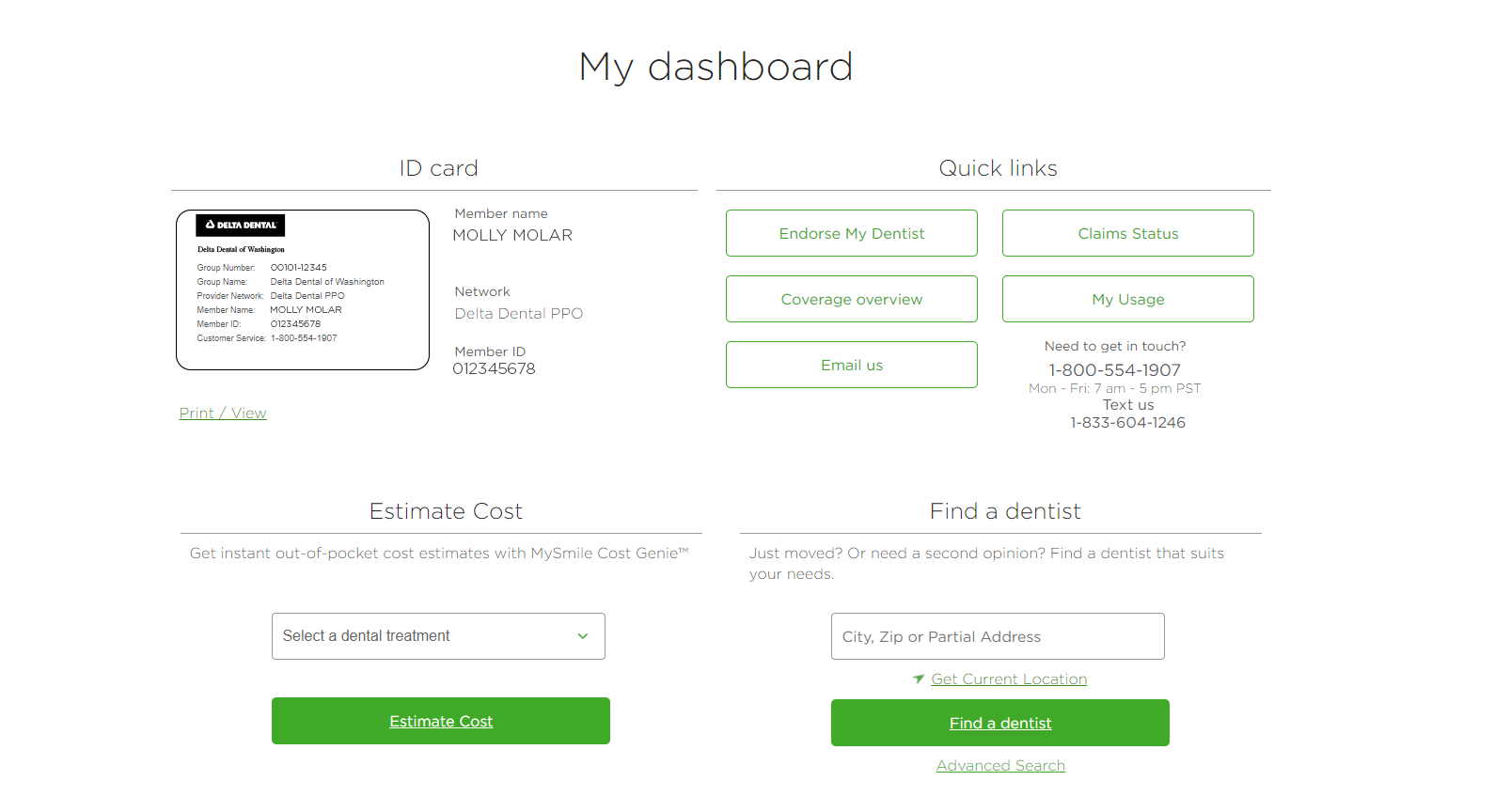
Dental Benefits Guide How To Check The Status Of Your Dental Claim Delta Dental Of Washington
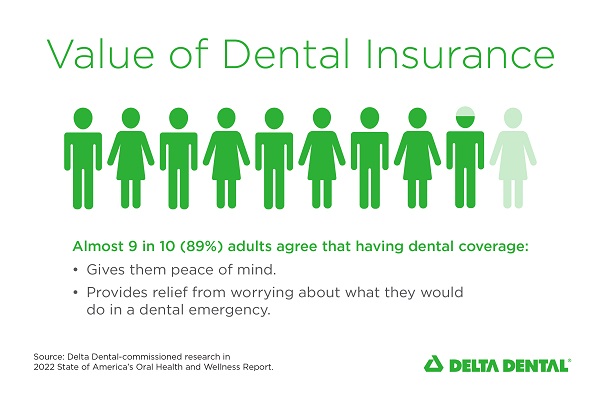
Dental Insurance Gives Peace Of Mind According To Delta Dental Study
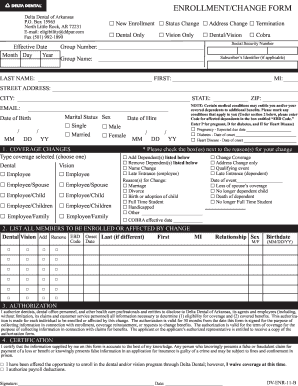
Delta Dental Enrollment Change Form 3400 Ca Fill Online Printable Fillable Blank Pdffiller